



Weekly M&M | May 22, 2025
Magic Mushroom Chemistry, Ketamine & the Opioid System, Cold Memories, History of the Hippocampus, Lipid Biomarker Data


Newest Episodes:
Last episode: “Linoleic Acid, Seed Oils, mTOR & Breast Cancer“ | Nikos Koundouros, PhD & John Blenis, PhD | [Listen here]
Current episode: “Psilocybin & MDMA: Inflammation, Stress & Brain-Body Communication” | Michael Wheeler PhD | [Listen here]
Next episode: “Psychedelic Chemistry, Magic Mushrooms, Kratom, Gray Market Research Chemicals, Vape Shops“ | Andrew Chadeayne, PhD | [Listen here]
Upcoming Guests:
TBD
Top Articles of 2025 (so far):
Bathing in Estrogen: Chemicals in many foods and consumer products disrupt estrogen signaling. The structure of the estrogen receptor explains why there are so many.
mRNA Shots & Acquired Immune Deficiency: A new study shows that mRNA shots can result in concerning immune system abnormalities.
Case Study: To statin or not to statin?
Research Highlights
I highly recommend the new episode with chemist Andrew Chadeayne. He does really cool work in psychedelic chemistry, such as characterizing molecules found in magic mushrooms beyond psilocybin/psilocin. Here’s one example:

Cool rodent study on “cold memories”: “We report that if mice are returned to an environment in which they previously experienced a 4 °C cold challenge, they increase their metabolic rates regardless of the actual environmental temperature. Furthermore, we show that mice have increased hypothalamic activity when they are exposed to the cold, and that a specific network emerges between the hippocampus and the hypothalamus during the recall of a cold memory.”

New evidence that the effects on ketamine in the brain depend in part of the opioid system. I spoke to the senior author about this topic on M&M 147.

As always, use this content to access studies behind a paywall.
Something Interesting to Watch:
My recent conversation with Dr. György Buzsáki is a good one to watch for neuroscience aficionados. In this clip, he describes the history of some key discoveries about the hippocampus, including “place cells” that appear to encode animals’ location in space.
READ THIS if you enjoy M&M and want to learn how to provide support.
Biomarker Data:
The data below are biomarker data from at least one individual and how I personally think about them.
Note: M&M content is NEVER medical advice. This should not be taken as a substitute for professional medical advice. Always consult a physician about your experiences and data before making health-related decisions.
Try SiPhox Health—Affordable at-home blood testing. Comprehensive set of key health markers in an easy-to-read dashboard. Code TRIKOMES for a 20% discount.
Here’s a basic lipid panel from an adult male in his late 30s, who reports being very active and in good metabolic health, eating a mostly whole food diet with these basic characteristics:
Relatively high in fat but low in PUFAs.
Somewhat low in carbohydrate (but not ketogenic), low in grains generally.
High in protein, mostly from animal sources like red meat, fish & seafood, and moderate dairy.
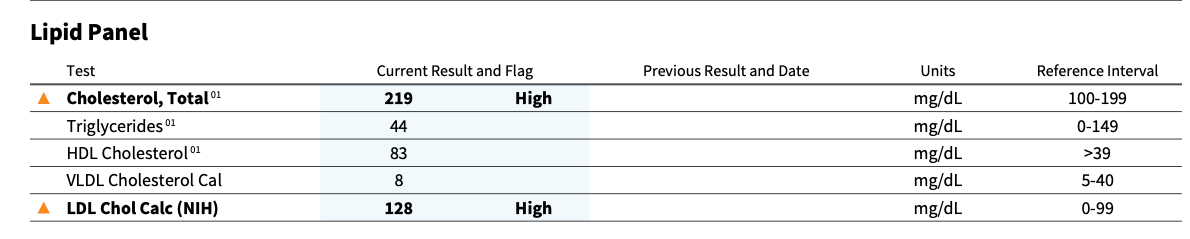
Take a moment to read these numbers, and notice that the Total and LDL-C levels were automatically flagged as “High” in the report. Notice also the following things:
Triglycerides are not elevated (often seen in fatty liver / poor metabolic health)
Triglycerides:HDL ratio is 0.53, consistent with very good metabolic health (a value close to or <1.0 is widely considered good, and 3+ not good)
vLDL is low, which is good (LDL particles come in two major forms, with the vLDL being the truly bad ones. See M&M 140 for more detail here)
The values are flagged as “High” for Total and LDL-C because they’re above the “reference interval.” Basically, those numbers are higher than what medical guidelines say is “optimal,” which I and many others scoff at. I wrote about cholesterol and statins here, based on some lipid data a menopausal women shared with me. In that case, her doctors were telling her what doctors would likely tell me: get on a statin to lower your “high” cholesterol.
But is TC = 219 and LDL = 128 “high” for an adult male in his late 30s? Well, here’s what the data say about mortality risk (see this article for source):

The LOWEST mortality risk for a male in this age cohort is… just over 220. So a TC of 219 is just about ideal, at least if you care about, uh, not dying.
What about LDL? Here’s age- and sex-adjusted data:

Based on that data, the lowest mortality risk is associated with LDL in the 132-154 range, so the male with LDL = 128 is most definitely NOT “too high,” based on these data.
What would you do in this person’s shoes?