



mRNA Shots & Acquired Immune Deficiency
A new study shows that mRNA shots can result in concerning immune system abnormalities.

Not medical advice.

We all had to decide whether to get the original COVID shots. What about boosters? Questions we all must grapple with—what to do, and why?
Practical questions like these require continual reappraisal as the evidence accumulates. If you’re like me, you constantly update your beliefs over time. As described in more detail here, my original conclusion regarding the Pfizer and Moderna shots was to get the initial two-shot injection. In early 2021, I believed the SARS-CoV-2 infection was a much greater risk to my health than it turned out to be. I was also excited by the new mRNA-based biotechnology, promising a new, rapidly reprogrammable platform by which we could immunize the entire world against novel pathogens.
My beliefs had begun shifting considerably before the first boosters were offered. For starters, I got sick with COVID just a few months after getting the double dose I was assured would prevent infection. As I learned more about the mRNA technology and parsed the doublespeak used to sell it to society (“100% effective,” the CEO of Pfizer proudly told the world), my beliefs changed. I’ve opted not to get any booster shots.
A new preprint from some high-profile Yale researchers has reaffirmed my decision to avoid boosters. You will have to make your own choices. My purpose here is to point you to some new information, briefly describe some key results, and connect the dots between this work and other things. I’m happy to share my own thoughts and how they guide my choices, but it’s not my style to try and convince you that you should or shouldn’t do something. We’re all adults here.
The new study conducted by some well-known and respected researchers from Yale: Immunological and Antigenic Signatures Associated with Chronic Illnesses after COVID-19 Vaccination
I’m not going to do a complete breakdown of this work but will highlight some of the specific findings and how some of the results fit into the bigger picture. Let’s start with the abstract itself (emphasis added):
COVID-19 vaccines have prevented millions of COVID-19 deaths. Yet, a small fraction of the population reports a chronic debilitating condition after COVID-19 vaccination, often referred to as post-vaccination syndrome (PVS). To explore potential pathobiological features associated with PVS, we conducted a decentralized, cross-sectional study involving PVS participants and healthy controls enrolled in the Yale LISTEN study. Compared with controls, PVS participants exhibited differences in immune profiles, including reduced circulating memory and effector CD4 T cells (type 1 and type 2) and an increase in TNFα+ CD8 T cells. PVS participants also had lower anti-spike antibody titers, primarily due to fewer vaccine doses. Serological evidence of recent Epstein-Barr virus (EBV) reactivation was observed more frequently in PVS participants. Further, individuals with PVS exhibited elevated levels of circulating spike protein compared to healthy controls. These findings reveal potential immune differences in individuals with PVS that merit further investigation to better understand this condition and inform future research into diagnostic and therapeutic approaches.
Recall how the COVID mRNA technology works: the Moderna and Pfizer shots contain mRNA encoding the SARS-CoV-2 spike protein, which is toxic. You want as little spike protein in your body as possible. A natural SARS-COV-2 infection and mRNA shots will expose you to spike protein. The hope with the shots is that by inducing some spike protein expression, your body will produce an immune response that makes any subsequent natural infection less severe, resulting in a lower overall spike protein exposure. The aim is more or less to reduce one’s total lifetime spike protein load.
In a perfect world, that immune response generated from the mRNA shots would prevent future SARS-CoV-2 infection. This obviously did not happen. In fact, there’s evidence that people who receive boosters are more prone to infection. Even though they didn’t prevent infection, the shots did reduce the likelihood of severe COVID—granted, most people are not at risk for severe COVID, but those with comorbidities like very age and poor metabolic health are.

Similar written content:
A metric by which we can judge the shots is how much total spike protein one is exposed to from an mRNA shot + natural infection compared to natural infection alone. In my case, I got the initial two-dose Pfizer shot, then got COVID anyway. The question for me is: was my total spike protein load from the shots + infection greater than or less than it would have been if I had skipped the shots before getting infected? The first hint came from my own visceral experience after the second dose: I was sick for several days.
We want to know if the mRNA shots produce “just enough” spike protein to initiate an immune response that at least helps prevent severe COVID, which would naturally come with a large spike protein load. On the other hand, if the mRNA shots produce “too much” spike protein, then perhaps the spike protein load from shots + infection is greater than what we would experience from a natural infection alone. That latter is plausible given that most people infected by SARS-CoV-2 experience mild symptoms, not severe COVID.
In any case, keep in mind the simple fact that the spike protein is toxic. You want to minimize your exposure. There’s no situation where spike protein exposure is good for your health. And you certainly don’t want spike protein to persist in your body for long periods of time. The worst case scenario would be a situation where each shot exposes you to significant spike protein levels, you repeatedly get infected by SARS-CoV-2 anyway, and each exposure poses risk for persistent, long-term spike protein expression in your body. Imagine someone who gets boosted and infected each year, with spike protein always circulating in their body, stimulating inflammation and tissue damage. Not good.

The new preprint contains data on people who received mRNA shots who were confirmed to have no prior SARS-CoV-2 infection, a key cohort for assessing whether mRNA can ever trigger “too much” spike protein expression. If severe and negative immunologic effects can be generated by spike protein induced by shots alone, then we have a problem.
Before looking at the new preprint, let’s review some background on what we’ve learned over the past few years…
Spike Protein & mRNA Technology: Some stuff we learned
Three years ago, people were already pointing out how the engineered mRNA shots presented a risk for spike protein persistence. In short, the use of pseudouridine residues in the synthetic mRNA found in the shots, together with their encapsulation in lipid nanoparticles, allows the synthetic mRNA to last much longer in the body than a natural mRNA molecule. I discussed and wrote about the possibility of spike protein persistence in this content, back in February 2022:
Podcast: Genomics, PCR, COVID Testing, mRNA Vaccines, Blockchain Technology, Cannabis & Psilocybin Mushroom Genomes | Kevin McKernan
Article: Pseudouridine, mRNA Vaccines & Spike Protein Persistence
Kevin McKernan has been consistently ahead of the mainstream curve on this stuff. Back in early 2022, he sounded the alarm about how the engineering details of the mRNA shots might lead to persistent spike protein expression and generate non-natural variations of spike protein with unknown biological consequences. In December 2023, almost two years later, there was experimental demonstration of McKernan’s worries. I wrote more about that here.
Since then, it has been shown that that the payload of the mRNA shots, synthetic mRNA molecules encapsulated in lipid nanoparticles, do not stay confined to injection sites (as we were originally assured). From this work, we know clearly that spike protein is often distributed throughout the body, to tissues like the heart and brain, where it can persist. Given that this stuff is specifically engineered to have artificially high longevity within our tissues, it’s hard not to wonder whether everything from myocarditis (heart inflammation) to the “brain fog” and other symptoms of “long COVID” are, to some extent, all side effects of the novel mRNA technology we injected into billions of people (after granting legal immunity to the manufactures).

In addition to those problems, McKernan and others have demonstrated that some of the mRNA vaccine vials were contaminated with pieces of DNA, which should not be in the shots at all. Even more concerning: this DNA can contain something called an SV40 promoter, an infamous DNA sequence which may pose a cancer risk. If you want to learn more about this, follow Kevin’s work here. Let’s just say that the idea that this stuff might be able to integrate into the DNA of human cells and promote cancer is looking less and less like a “conspiracy theory” every week.
Related M&M podcast content:
M&M #196: Vaccine Contamination & Fiat Science | Kevin McKernan
New Preprint Study Basics
The new study examined blood samples from several dozen human patients taken between late 2022 and 2023. Based on vaccine histories, each patient had received 0-4 doses of a COVID shot (most were the Pfizer/BioNTech or Moderna versions).
They also had to determine patients’ SARS-CoV-2 infection history. Because asymptomatic infections are common, they had to confirm via blood tests whether people had any previous infection. Bottom line: they did testing that allowed them to categorize people based on their vaccine and infection history. The four basic patient groups they compared were:
Vaccinated 1+ times, with prior SARS-CoV-2 infection
Vaccinated 1+ times, no prior SARS-CoV-2 infection
Not vaccinated, with prior SARS-CoV-2 infection
Not vaccinated, no prior SARS-CoV-2 infection
Here’s a graphical breakdown from the preprint, showing that there were 11-27 people per group:

They ran a bunch of tests on patient blood samples, enabling them to not only determine prior SARS-CoV-2 infection history but also look at different aspects of the immune system, such as inflammatory markers and levels of white blood cells.
Some of the vaccinated patients had reported “post-vaccination syndrome” (PVS), a constellation of symptoms experienced sometime after receiving a shot. Were those symptoms truly induced from the vaccine, or might they be from a prior and possibly asymptomatic infection? The bloodwork enabled researchers to parse this. They could isolate patients who reported PVS and verify that they had zero prior SARS-CoV-2 infections. Thus, if the mRNA shots are capable of inducing PVS independent of SARS-CoV-2 infection, they will see evidence of it in that particular subset of patients.
A description of the “post-vaccine syndrome” that people reported—notice that PVS sounds a lot like what people refer to as, “long COVID”:
The most frequent symptoms reported by participants were excessive fatigue (85%), tingling and numbness (80%), exercise intolerance (80%), brain fog (77.5%), difficulty concentrating or focusing (72.5%), trouble falling or staying asleep (70%), neuropathy (70%), muscle aches (70%), anxiety (65%), tinnitus (60%) and burning sensations (57.5%).
Here’s what reported symptoms looked like for each of the four groups. “Control” here mean those that did not report post-vaccine syndrome after getting shots, either with or without prior infection. The red and blue bars are those would did report PVS—red is vaccinated people without prior infection, blue is vaccinated with prior infection.

Notice that the red and blue bars differ from the control (gray) bars. This indicates that, on average, patients that reported PVS had more anxiety, depression, etc. whether or not they had prior infection. In other words, symptoms of PVS were present in some people who received COVID shots but had zero prior SARS-CoV-2 infections (red bars). Notice also that the red and blue bars are not statistically different from each other. This indicates that, on average, PVS symptoms were just as strong in PVS patients without prior SARS-CoV-2 infection as they were in those that had.
How did the immune systems of PVS patients look? The headline results from the abstract state that, “Compared with controls, PVS participants exhibited differences in immune profiles.” These included:
Reduced circulating memory and effector CD4 T cells.
An increase in TNFα+ CD8 T cells.
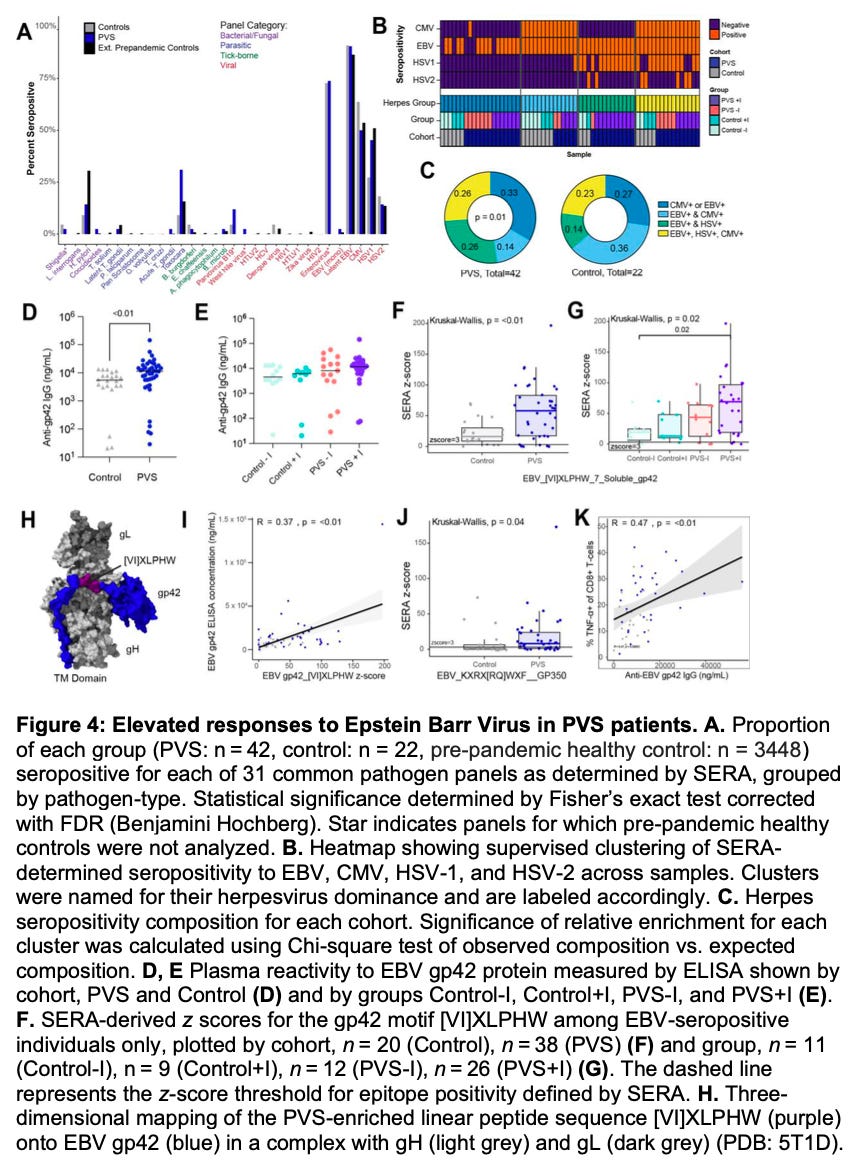
More infrequent serological evidence of recent Epstein-Barr virus (EBV) reactivation.
CD4 T cells are a type of white blood cell that help fight infection. In general, you do not want to have reduced levels of CD4 T cells. TNFα+ CD8 T cells are another type of immune cell that produce the potent inflammatory cytokine TNFα (“tumor necrosis factor alpha”). You generally do not want a persistent elevation in these cells, which would indicate prolonged inflammation. EBV is a common virus whose activation results in symptoms quite similar to those reported in PVS and “long COVID.”
Here’s what some of the data actually looks like for immune cell levels:

And for Epstein-Barr virus (EBV):
Do COVID shots induce long-lasting spike protein expression?
Here’s the punchline: in patients who reported post-vaccination syndrome (PVS), spike protein could be found in plasma 26-709 days from their most recent exposure. In other words, some PVS patients had detectable spike protein up to two years post-vaccination. In PVS patients, whether or not they had a prior infection, only a subset of patients had detectable spike protein “long” after their last exposure. Nonetheless, these data show that it’s possible for spike protein to persist for months or even a couple years in people, including those who received an mRNA shot and confirmed to never have had prior SARS-CoV-2 infection.

Here, I wrote about previous work that was able to detect vaccine mRNA in the lymph nodes of patients up to 60 days after the second dose of the Pfizer shot. In that study, they also measured spike protein levels in samples from patients who died of severe COVID, finding that spike levels were actually lower in those patients than those who received an mRNA shot. Collectively, these results are consistent with what I and many others experienced from the two-dose shot: we got pretty damn sick, suggesting that the mRNA shots often induce high levels of spike protein production.
Putting it all together, what seems to be happening is that, as a consequences of how the mRNA shots are engineered, the artificially stabilized mRNA results in long-lasting spike protein production in some people. Why only some people? And why does the length of spike protein persistence vary so much from person to person? There are several factors that likely contribute to. One is natural variation. Maybe your ribosomes tend to produce more protein from mRNA than mine, or vice versa. I suspect sex and age come into play here. One reason why myocarditis is seen more in young men than other demographics may be because protein production is generally cranked up higher in that demographic. To the extent that’s true, more spike protein would be produced, increasing the likelihood of negative effects.
Another factor is dumb luck. The shots are supposed to be intramuscular. By chance, the nurse giving the shot might happen to hit a blood vessel, injecting lipid nanoparticle encapsulated mRNA into your bloodstream. In that case, spike protein mRNA is pumped throughout your body. Depending on where it goes and how much there is, this can affect expression duration. We already know from this recent work that this stuff can end up all over the body, far away from the injection site.
When you think about the bioengineering of the mRNA shots, long-term spike protein production makes a lot of sense. The mRNAs are synthetic, containing unnatural residues that stabilize the mRNA, by design. They are further protected from degradation by the lipid nanoparticles, further enabling them to spread beyond the injection site.
To the extent there’s persistent spike protein expression, you would expect it to trigger inflammation. Spike protein is a toxic, foreign substance that the body wants to destroy. That’s the purpose of inflammation. The longer spike protein persists or the more there is, the more inflammation there will be. It’s not surprising PVS patients had higher levels of TNFα+ CD8 T cells. Those cells promote inflammation. Makes sense.
What’s a bit more puzzling is why post-vaccination syndrome patients were observed to have lower circulating memory and effector CD4 T cells. That is an immune system deficiency. In fact, there’s an infamous condition named after its association with low CD4 T cell levels: Acquired Immune Deficiency Syndrome (AIDS).
Can COVID shots lead to an acquired immune deficiency?
You can spend as much time as you want jumping down an HIV/AIDS rabbit hole. Plenty of people have. If you’re interested, reading the words of Kary Mullis is a good place to start (e.g. the forward he wrote to this book). He won a Novel Prize for inventing PCR, a technology used in every molecular biology lab today. PCR tests were widely used during the HIV/AIDS epidemic of the 1980s and the COVID era to detect viral infections. Mullis is simultaneously regarded as one of he most brilliant scientists of his generation and “wacky” because he was an “AIDS denialist.” Like many students, I believed this for a long time, simply because it’s what I was told. It wasn’t until recently that I actually read Mullis directly on the subject.
To my horror, I discovered that his “denialism” was nothing more than asking one of the simplest and most fundamental questions in science: what is the evidence for that? He asked researchers in the field to share papers the demonstrated that HIV was necessary and sufficient to cause AIDS (on its own). He did not find that evidence compelling. Whether or not you agree with this stance, there’s nothing wacky or unscientific about it. It’s commonplace for scientists to find published work unconvincing (very commonplace), especially when big, bold claims are being made (and generating incredible cash flows).
Anyways, I digress.
My purpose here is simply to point out the curious CD4 T cell deficiency observed in this study. How do our major health institutions currently define AIDS? Here’s a definition from hiv.gov:
A disease of the immune system caused by HIV. HIV destroys the CD4 T lymphocytes (CD4 cells) of the immune system, leaving the body vulnerable to life-threatening infections and cancers. Acquired immunodeficiency syndrome (AIDS) is the most advanced stage of HIV infection. To be diagnosed with AIDS, a person with HIV must have an AIDS-defining condition or have a CD4 count less than 200 cells/mm3 (regardless of whether the person has an AIDS-defining condition).
So, a count of your CD4 T cells is the basic criterion used to diagnose AIDS. If it falls below that threshold, you can be diagnosed with AIDS.
So did any of the PVS patients in the new preprint study have AIDS? One of the features of PVS patients they measured was, “reduced circulating memory and effector CD4 T cells.” Here’s what they say for PVS vs. non-PVS patients, in terms of the levels of various T cells:

For three of the CD4 T cell cell subtypes, PVS patients had significantly lower levels than controls (on average). Were levels ever low enough to satisfy the AIDS definition? I’m not sure. The data in the paper are expressed in percentage terms, rather than cell counts. But the point is that what we’re looking at here is a form of immune deficiency, which patients acquired after receiving mRNA shots.
I don’t want to speculate or read into this too much, but the immune deficiency phenotype fits with this data, which shows that the chances of SARS-CoV-2 infection actually go up as people receive more booster shots:
You can draw your own conclusions, but this data makes me glad I chose not to get mRNA booster shots. After the second dose of the original two-dose Pfizer shot I was sick for a few days. I don’t recall ever getting ill after a shot before in my life, and the shot-induced symptoms I experienced were strong—much stronger than what I experienced several months later, when I got COVID anyway—implying that the shot induced substantial spike protein production in my body.
At this point there are a large number of people out there who have received three, four, and even five or more doses of these mRNA shots. Do you or anyone you know keep getting COVID boosters? Are you experiencing symptoms of “long COVID” or something similar?
If so, perhaps you should get your CD4 T cell levels checked.
You’re not an AIDS denialist, are you?
Interesting, but flawed analysis of the pre print.
Best decision I ever made. I mean when did all of a sudden did we as a society forget that Pharma is a legal mafia that kills people as part of its business plan, pays a fine and pockets the remaining 95% of the profit of said drug?