



Spike Protein Persistence, Experimental Design & Rushed Science
When reading studies, do not take the conclusions at face value just because of “statistical significance.”

Not medical advice.

Many people have reported symptoms, including neurological symptoms, long after getting COVID. One good candidate explanation for how symptoms might persist long after the initial sickness is spike protein persistence. The spike protein is an essential component of the SARS-CoV-2 virus, enabling it to infect our cells. The mRNA in the Pfizer and Moderna shots encodes this protein.
(Those shots are supposed to contain specially engineered mRNA molecules encased in lipid nanoparticles without any DNA. It’s now been shown that many vials have been contaminated with residual DNA encoding other things—oops!)
As I’ve previously written, the spike protein is cytotoxic. Suppose spike protein gets into your body, either from natural SARS-CoV-2 infection or a synthetic mRNA injection. You want your immune system to detect it, clear it out, and retain an immune memory in order to mount a fast, robust response to any future infection. You do not want the spike protein to persist longer than is necessary to generate a sufficient immune response.
No matter what strategy you’ve taken with COVID shots and infection, everyone shares a common interest: minimize the total amount of spike protein in your body and how long it’s inside you. The more spike protein you’re exposed to, the worse off you will be.
What’s the best way to minimize spike protein exposure? It depends on who you ask.
Related M&M content:
Article: Pseudouridine, mRNA Vaccines & Spike Protein Persistence
Podcast: Vaccine Contamination & Fiat Science
Some say that getting mRNA shots (and boosters) is the way to go because it will reduce how much spike protein you get from any subsequent infection. And as we all now know, you probably will get infected at some point, no matter how many shots you’ve received—the argument is that those future infections will produce much less spike if you’re already vaxxed. There’s evidence that the shots protect against severe illness, which implies that spike protein production from subsequent infections might be lower than it would have otherwise been. The implicit assumption here is that your total spike protein exposure from vaccination plus subsequent infection will be lower than from infection alone.
Below, we will examine and critique a recent paper making the above argument.
Another line of reasoning holds that mRNA shots, especially repeated doses (boosters), will likely cause high levels of spike protein exposure on their own. The synthetic mRNA in the Pfizer and Moderna shots has been engineered to enhance mRNA stability, which is why both the mRNA and the recombinant spike protein can be detected in people many weeks after vaccination, including in tissues far away from the injection site. If you’re going to get infected anyway, then each shot and each infection amount to separate spike protein exposures stacked on top of each other. There’s even evidence that receiving more boosters is associated with higher rates of infection from emergent virus strains. To the extent that’s true, continual booster shots would likely result in higher lifetime spike protein exposure than natural infection on its own.

Whatever your thoughts or personal strategy, the important thing to remember here is the overall spike protein exposure. More spike exposure is bad. We want to consider how to minimize this and whether the specific experimental results below offer a clear and compelling answer.
Again, spike protein exposure will result, to some degree, from both natural infection and mRNA shots. If the mRNA shots are effective in reducing overall spike protein exposure, they must result in much lower spike protein production in infections that occur after vaccination (without also increasing the odds of future infection).
There’s also the issue of how long spike protein persists after infection vs. vaccination, which ties into the issue of long COVID…
Want to do your own research?
Research question: How long does SARS-CoV-2 spike protein persist in the body after vaccination vs. infection?
Study: Effectiveness of the Coronavirus Disease 2019 Bivalent Vaccine
Long COVID & Spike Protein Persistence
A leading hypothesis for why some people report persistent COVID symptoms is that the spike protein persists in the body longer than it’s supposed to. There are multiple ways one can conceive of this happening. One is that the body fails to degrade or clear out spike protein molecules as quickly as it should—you get a viral infection, but the spike protein persists even after the virus has otherwise been cleared out.
Another possibility is persistent spike protein production rather than a clearance failure. How might this happen? For me, this scenario is much easier to imagine for vaccination. As reviewed elsewhere, the mRNA contained in the shots is not native viral RNA. Instead, it’s modified spike-encoding mRNA engineered to be much more stable than natural mRNA molecules. This stability is achieved by using special “letters” in the RNA code and encasing the mRNA molecules within protective bubbles (lipid nanoparticles). By design, this prevents mRNA molecules in the Pfizer and Moderna shots from degrading as rapidly as natural RNA. A possible side effect of this enhanced stability could be longer-lasting spike in protein production.
I discussed the possibility of spike protein persistence with Kevin McKernan on M&M #58, back in February 2022. He also described the possibility that the synthetic mRNAs from Pfizer and Moderna might be able to produce more than just native, viral spike protein. In 2023, clear evidence emerged for this—“ribosomal frameshifting” results in the production of other proteins similar to native SARS-CoV-2 spike, with unknown consequences. Do these potential mystery proteins trigger stronger immune reactions or perhaps linger in the body? As far as I’m aware, no one knows.
From studies like this, we know that in people who received two doses of the Pfizer shot, synthetic mRNA was detectable in the lymph nodes of most people two weeks after the second shot and as late as 60 days later in some samples. If that’s possible after two shots, how much total spike exposure might there be after three or more shots? I’m not exactly sure, except that getting more shots will inevitably mean more exposure. (Please share in the comments any studies that have measured spike levels after multiple shots).
A new study has investigated the phenomenon of spike protein persistence and its connection to long-lasting inflammation and neurodegeneration-related changes in the brain. Below, I will briefly summarize what they found before pointing out some curiosities in the data. With sufficient experience reading scientific papers, you develop an eye for data and experimental conditions that are absent, even though they would have been highly informative…
New Study: “Persistence of spike protein at the skull-meninges-brain axis may contribute to the neurological sequelae of COVID-19”
The main findings of this new study will be described very briefly below. In essence, the paper reaffirms that spike protein can persist in the body for longer than we might like and expands our knowledge of exactly what goes wrong as a consequence. They show that spike protein persists in the nervous systems of both humans and mice, causing long-lasting neurological problems. This could explain long COVID symptoms.
Here’s the authors’ own summary, in graphical abstract form:
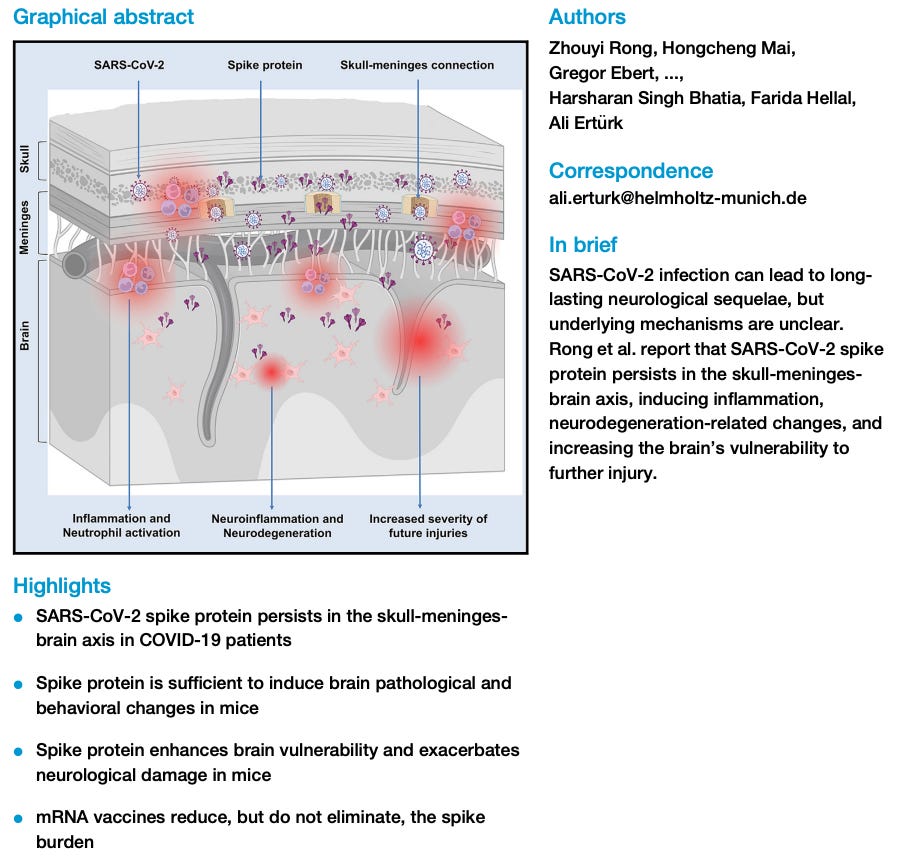
After SARS-CoV-2 infection in humans, spike protein can be found in the skull-meninges-brain axis long after viral clearance from the body. Spike protein was found in post-mortem brain tissues of COVID patients. They also detected evidence of things like micro-bleeds in brain tissue and markers of neurodegeneration in these patient samples. If cytotoxic spike protein sticks around in brain tissue, you’d expect to see some sign of tissue damage, which they confirmed.
Mouse studies were then used to understand better what spike protein actually does. Main findings include:
SARS-CoV-2 infection in mice leads to proteomic changes reminiscent of those seen in post-mortem human tissue samples. Basically, different protein pathways get up- or down-regulated, including those involved in inflammation.
When pure spike protein is injected directly into the skull, you see neuroinflammation. This means that the spike protein by itself, rather than other viral components, can account for most of the observed issues.
Spike protein injected into general circulation leads to proteomic changes in the brain (dysregulated protein function) and “anxiety-like” behavior in mice. In other words, spike protein not only leads to physical damage to brain tissue but measurable behavioral effects reminiscent of those reported in long COVID.
The presence of spike protein in the brain exacerbates other forms of neurological damage. For example, if mice have a stroke, the damage done is worse if there’s spike protein in their brain when it happens.
Injecting mice with two doses of Pfizer mRNA shots before SARS-CoV-2 infection has a “protective effect” against spike protein accumulation—mice that receive COVID jabs before viral infection show lower levels of spike protein and inflammatory markers, compared to mice who are infected without prior vaccination.
It’s this last observation I want to dig into, as there are some interesting omissions from this study that prevent us from taking the authors’ interpretation of the data to the bank. Remember: spike protein is toxic. All other things being equal, the more total spike protein in the body, the more damage will be done.
The results of this study clearly show that vaccinating before SARS-CoV-2 infection results in lower levels of viral proteins (including spike) in the mouse brain, as well as lower levels of one inflammatory marker (IL-6). Here’s the data:

Stare at these graphs. Notice what’s present. Notice what’s absent. Are there any conditions missing that might be informative? Other key details to keep in mind when evaluating results like this:
Exactly when were the measurements made relative to the manipulations? Would you expect the timing to impact the measured outcomes?
How many data points are in each group, and how variable are the measurements from one individual to the next? Don’t assume that “statistical significance” means the results are robust.
Are there any logical experimental conditions that are absent, especially controls? Why might this be, and what might those results have been?
Let’s scrutinize these results in more detail…
Critically Evaluating Scientific Published Results: Sparse data, timing & “statistical significance”
From these experiments, we’re essentially trying to understand which combinations of vaccination and infection produce the highest overall levels of spike protein production. Two complementary ways to measure the amount of spike protein production: peak spike protein levels at any given time, or the total amount of spike protein production over time. To measure either of these definitively, one would need a time series of measurements—ideally, you would measure spike protein levels at multiple time points after some manipulation (vaccination, infection) and fit a curve to the results. With this data, you could do two things: (1) look at peak spike protein levels, wherever it may be in the time series; (2) calculate the “area under the curve,” total spike protein over the entire interval.
Of course, time and resources are limited. Scientists often can’t make all the measurements they might want to. Experiments take time, effort, and money. There’s also a natural incentive to publish results ASAP, especially in hot fields like COVID.
Experimental time course
The first thing to notice is that measurements of spike protein levels and inflammatory markers in this study were made at a single time, providing one snapshot of spike protein and IL-6 levels. From the graphs, we do not know what spike protein or IL-6 levels looked like before or after this single time point.
When, exactly, were these measurements taken? Mice were sacrificed five days after SARS-CoV-2 infection, which itself took place ten days after the second of two mRNA shots. The first shot was given four weeks before that. So for each mouse, this was the timeline:
On day 1, they receive their first injection (mRNA shot or control).
4 weeks (28 days) later, they receive the second mRNA shot (or not).
10 days later (38 days from the start), they’re infected with SARS-CoV-2 (or not).
5 days later (43 days from the start), they are sacrificed, and the measurements in the graph above were taken.
So, the gap between the two shots is much larger than the total interval of time encompassing the second shot, subsequent infection, and end of the experiment—28 days vs. 15 days. Think about when spike protein will be produced along this timeline. Some amount will be produced after the first shot, some after the second shot, and some after infection. The total amount produced will vary for each condition and across time.
There will also be an interaction between the shot and infection in mice that received both. That’s what panel 7E above shows us: for mice that got two shots before being infected, spike protein and IL-6 levels were lower than in mice that were infected without prior vaccination. We have no idea what those levels were at any previous time point, including the four weeks between the two shots or the ten days after the second one but before infection.
That’s a critical point. For the mice that did not receive prior vaccination, they are plotting spike protein and IL-6 levels shortly after those animals had their very first wave of spike protein. For the animals that received two shots before infection, the first encounter with spike was over a month earlier, when they received their first shot. In any animal, under any of these conditions, we expect the first encounter with spike to result in the most spike production. But that’s not what those graphs are comparing. The bar plots above compare spike protein and IL-6 levels in one group of mice that just had their first spike exposure (infection-only animals) to those who just experienced their third exposure (two doses of shots, then infection).
Spike protein levels would have gone up to some extent in response to each of the two vaccine doses. By how much? We have no idea. We know that spike protein levels did not go up as much following infection in mice who have been previously vaccinated, but we have no idea how much spike protein was produced in the vaccinated mice right after the first or second shot. What if either of the shots produced more spike protein than was seen in non-vaccinated animals following SARS-CoV-2 infection? That would completely change our interpretation of this figure.
In my view, what we really want to know is whether the total cumulative spike exposure from two shots + infection was higher or lower than from infection alone. Given the human data mentioned above, showing that synthetic mRNA and spike protein from shots can persist for weeks in humans, it seems very plausible that two shots + infection could produce more total spike protein exposure than a single infection.
But again, there’s no way to assess that from these experiments.
Experiments not done
Another thing to consider is that we are missing some logical experimental conditions. The first is a vaccine-only group—mice that get a two-dose shot but no subsequent SARS infection. Another is SARS infection before vaccination. These are relevant, real-world conditions. The researchers presumably did not do these experiments. (It’s also possible that they did them but omitted the results for some reason).
I asked the senior author, who told me this:
“We focused our experiments specifically on the conditions relevant to understanding the toxicity of the spike protein arising from infection. The study design did not include the additional conditions of vaccine + no infection or infection + subsequent vaccination. The rationale for this choice was the Focus of the Study: The primary aim was to investigate spike protein toxicity in the context of infection. Vaccination and vaccine-related toxicity were beyond the scope of this work, as infection typically produces spike protein loads that are orders of magnitude higher (millions to billions of times) than those induced by vaccination.”
—Dr. Ali Ertürk
I was particularly struck by the final claim: “infection typically produces spike protein loads that are orders of magnitude higher (millions to billions of times) than those induced by vaccination.” However, I have not seen direct evidence of this in my reading of the literature so far. Then again, there’s a lot out there, and I may be missing something. I asked Dr. Ertürk to provide links to studies supporting his claim but have not received a response.
Update (Dec. 10, 2024): After sending two additional follow-up emails over the course of five days, I received this response from Dr. Ertürk:
I don’t have a reference; it was a guess based on millions dying from Corona—probably due to overproduction of the virus and its proteins, like spike.
Still, I presume there could be some ways to quantify this accurately, which we have not done.
Ok, so those experiments were beyond the scope of this work, the primary aim of which was “to investigate spike protein toxicity in the context of infection.” Why were they only interested in spike protein toxicity in the context of infection and not also vaccination—especially since, as mentioned previously, spike protein has been detected for weeks in human tissues post-vaccination? Beats me. But this is a fast-moving field. Time is money.
Again, experiments are hard, expensive, and time-consuming. They published the results above with just barely enough data points to see statistical significance. To me, this indicates that they wanted to publish quickly.
Which brings me to my next point…
In Figure 7, the two conditions in panel D have just three mice each. Three! The results are statistically significant at the magical p>0.05 threshold. But if you know anything about statistics, you’ll know that three data points are not enough to take the results to the bank, even if your calculator tells you it’s “significant.”
In panel 7D, the first two bars are from just four mice each. The third bar is from eight. The key comparison is the second and third bar, which is interpreted to mean that vaccination protects against inflammation, as IL-6 levels are lower in the vaccinated mice. The p-value for that comparison is 0.0485, just barely clearing the 0.05 significance threshold. Look at the plot again, closely:

Two of the four dots on the middle bar are within the range of dots on the third bar. In other words, the entire difference between the conditions here comes from just two mice that had especially high IL-6 levels. If they had run that condition with more than four mice, it’s likely that most (or all) of the additional data points would have been lower than those two high ones, which could have easily generated a non-significant result.
But why waste more time and resources to collect more than four data points if you’re already seeing “statistical significance,” especially if more data upsets this result? Time is money. Publish or perish. There is no incentive to collect that data when the first four data points give you this result.
Vaccination timeline & potential vaccine-only effects
It’s also strange to me that four weeks elapsed between the two mRNA shots. At first blush, this might seem sensible. After all, people who got the first two mRNA jabs back in 2021 were advised to separate doses by 3-4 weeks. This paper mimics that. But we’re talking about mice here—their metabolism is much faster than ours, which is why drugs have a very different time course in mice vs. humans. For example, psilocybin can induce multi-hour psychedelic trips in people. In mice, the effects last for minutes. Think about that in the context of the two-dose mRNA shots given in this paper. Following the first one, four weeks would presumably be more than enough time for spike protein levels to rise, peak, and fall again—all before the second dose and the subsequent infection. The initial shot obviously would have inevitably triggered a spike protein production to some degree, but the experimental design prevents us from knowing how much.
A vaccine-only condition would have at least allowed us to see if spike proteins or inflammatory markers were elevated above baseline in response to mRNA shots, which by design contain stabilized mRNA molecules capable of lasting longer than native viral mRNA. Yet another relevant condition not tested here is a third dose instead of infection after two doses. After all, official institutions recommend boosters to people, and millions of people have received three or more mRNA doses.
Again: time is money. Publish or perish. In my correspondence with Dr. Ertürk, he did acknowledge the importance of these conditions, and hinted at some ongoing work:
“That said, we acknowledge the importance of these additional conditions, particularly in understanding real-world scenarios involving vaccination and infection interactions. These are valuable questions to explore in future studies, and we hope they inspire follow-up investigations.
Additionally, we agree that vaccine off-target effects and delivery systems warrant detailed analysis. We are addressing these aspects in a forthcoming manuscript focused on nanocarriers and lipid nanoparticles, which will be published in January. This work will delve into off-target expression and the broader implications of delivery systems.”
Final thoughts
Given what we know about the stabilized mRNA found in the Pfizer and Moderna shots and the evidence of elevated spike protein in vaccinated humans, substantial spike protein production following the first and second doses of the mRNA shots seems very likely. However, this study didn’t measure spike protein levels after vaccination only (or any time point remotely close to the first shot).
The authors of this paper interpret the lower spike protein and IL-6 levels in animals vaccinated prior to infection to mean that the shots “protected” mice, implying that vaccination resulted in lower overall spike protein levels and inflammation. But their experiments only show that those things were lower at a single time point. It’s likely that vaccination induced substantial spike protein production and inflammation in the weeks leading up to the subsequent infection, such that the grand total was larger than for unvaccinated animals expose to SARS-CoV-2 for the first time. These experiments simply can’t tell us whether or not that’s true.
When I think about my own experience getting those first two Pfizer shots, I got quite sick from the second one (the only time in my life I’d ever been sick following a shot). That must have involved a substantial spike protein production. When I contracted COVID several months later, my illness was mild in comparison. Did the shots “protect” me by making the infection more mild? Sure, that’s likely. But it obviously did not prevent infection entirely, and so it means I experienced three waves of spike protein production over time.
Did those three waves of spike production expose me to less overall spike protein than if I had experienced a single wave from a natural infection?
I’m not banking on it…
To learn more, try these resources:
Podcast: Vaccine Contamination & Fiat Science | Kevin McKernan
Paper: Strategies for the Management of Spike Protein-Related Pathology
Research question: How long does SARS-CoV-2 spike protein persist in the body after vaccination vs. infection?
Try Consensus to do your own research. Use code MINDMATTERSPECIAL2 for a free, 1-year premium subscription.
Also missing from the data: how many mice died after the second shot and were simply excluded from the dataset altogether?